A hairy situation: How stress impacts hair loss
By Dr. Esha Singh, ND
Features Clinical Patient Care hair loss stress Telogen effluvium Photo: © Voyagerix / Adobe Stock
Photo: © Voyagerix / Adobe Stock If you search the term “stressed” in any internet browser, chances are you will be bombarded with images of all sorts of people pulling at their hair. While stress can manifest in many ways, there is some truth to that image – stress and hair health are deeply connected. In fact, stress, whether acute or chronic, is one of the leading causes of hair loss in adult populations around the world.
A primer on stress
Generally speaking, we as a society, are massively stressed out. Whether it is financial stress, relationships, work-life balance, or the fact that we are living through a pandemic, many of us are existing in an adrenaline-charged, fight-or-flight state. Whether a stressor is real or perceived, our body experiences a very real physiological response that is regulated by the HPA (hypothalamic-pituitary-adrenal) axis. This axis of communication is maintained by several critical hormones, including corticosteroid releasing factor (CRF), adrenocorticotropic hormone (ACTH) and cortisol (Lee et al, 2020).
When there is a stressor or triggering event, the hypothalamus is stimulated to produce CRF (Lee et al, 2020). CRF then acts on the CRF receptor on the anterior pituitary gland, which in turn produces proopiomelanocortin (POMC)-derived ACTH (Lee et al, 2020). Finally, ACTH acts upon the adrenal cortex to upregulate cortisol production (Lee et al, 2020). This increase in cortisol production increases glucose in the bloodstream and enhances the brain’s usage of glucose (Hoover et al, 2021). Additionally, it suppresses physiological processes that are cumbersome to the fight-or-flight state, such as digestion and reproductive processes (Hoover et al, 2021). When the stressor is removed, cortisol levels return to baseline and are maintained via negative feedback (Lee et al., 2020).
Telogen Effluvium
Telogen effluvium (TE) is one of the most common forms of diffuse hair loss, second only to androgenetic alopecia (Malkud et al, 2015, Asghar, 2020). The term effluvium is derived from Latin, meaning “to flow,” to infer that hair is flowing into the telogen stage (Malkud et al, 2015). It is characterized as a non-scarring form of hair loss that often presents three months after a triggering event. It can last up to six months and is self-limiting (Malkud et al., 2015).
Etiology and epidemiology
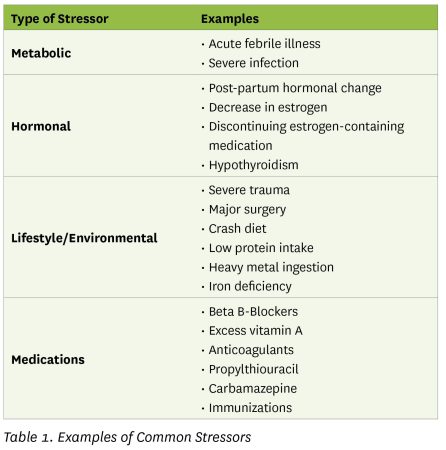
TE is a reactive process and is triggered by several stressors including metabolic stressors, hormonal shifts, lifestyle changes or certain medications (Hughes & Saleh, 2021).
TE can occur in individuals of all ages, ethnicities, and genders (Hughes & Saleh, 2021). Female patients, however, tend to experience TE more frequently than males due to more drastic hormonal changes throughout their lives (Hughes & Saleh, 2021). Female patients may also be more likely to notice and report hair shedding to their healthcare provider (Hughes & Saleh, 2021).
Anatomy and cycles
Hair is essentially made up of two structures: a shaft and a root. The shaft is what can be been on the surface of the skin, while the root is deeper down in the dermis and is surrounded by the hair follicle (informedhealth.org, 2006). The hair follicle is made up of mesenchymal-derived dermal papilla cells (DPCs) and epithelial-derived root sheets (Lee et al, 2020). The interaction between these two tissues regulates hair growth and development and maintains a normal hair cycle (Yang et al, 2010).
To understand telogen effluvium, it is important to first understand what the normal hair cycle looks like. While the hair throughout the body goes through the same stages, the duration of each stage differs depending on what part of the body you are focussing on (Hoover et al, 2021). Additionally, the rate of hair growth in individuals is influenced by many factors, including age, gender, and genetics (Hoover et al, 2021).
Skin is the largest organ of the body and up to 90% can be covered in hair follicles (Paus & Cotsarelis, 1999). The scalp portion of the skin has roughly 100,000 hair follicles and is one of the densest areas of follicles on the body (Saleh, 2021). The hair follicles undergo repetitive, regenerative cycles that consist of four stages: (1) anagen, (2) catagen, (3) telogen, and (4) kenogen (Avci, 2014). Anagen is an active stage, characterized by rapid growth. At any given time, about 90% of the hair follicles are in the anagen stage. This stage lasts between 2-6 years, with an average of three years (Saleh, 2021). During this stage, DPCs rapidly undergo mitosis, allowing for hair to grow 1/2-1 inch per month (Malkud, 2015). After anagen, the hair follicle transitions into the catagen stage. During this stage, the growth rate decelerates and the follicle prepares to go into the rest stage (Avci, 2014). This stage lasts about 10 days (Saleh, 2021). During the telogen stage, there is no growth. The follicle can stay at rest for 3-5 months (Saleh, 2021). At any given point, about 10% of hair follicles are in the telogen stage. The final stage of the hair cycle is another transitory stage, kenogen, during which the existing hair is shed and the follicle is empty (Avci, 2014). Under normal circumstances, one can lose up to 100 strands of hair per day.
Pathophysiology
In telogen effluvium, hair follicles shift prematurely into rest phase after acute or chronic stress (Asghar, 2020). Thom et al determined that stress can impact hair health and density in three main ways (Thom et al, 2016):
- Acute or chronic stress can induce hair loss
- Stress can worsen hair loss that initially caused by another condition
- Hair loss can cause increased stress due to feelings of shame and/or embarrassment
- For the purpose of this article, we will only look at acute/chronic stress inducing hair loss.
As aforementioned, whenever there is a stressor, whether physical, psychological, or environmental, the body upregulates CRF production. Interestingly, skin has been found to contain CRF, other HPA axis hormone analogues, and their receptors, indicating that there is neuroendocrine activity at the dermal layer (Arck et al, 2006). The presence of CRF has been found to simultaneously inhibit the elongation of the hair shaft and induce the premature regression of the hair follicle (Arck et al, 2006). This is achieved by arresting the cell cycle at the G2/M phase and increasing the accumulation of reactive oxygen species (ROS) (Lee et al, 2020). High levels of CRF also inhibits the proliferation of DPC, increases the production of reactive oxygen species, decreases growth-related molecules and increases regression-related molecules (Lee et al, 2020).
Additionally, the increase of substance P, a stress-related neuropeptide, is associated with premature hair loss (Peters et al, 20006). Substance P increases mast cell degranulation, increases number of entering the late stages of catagen, and inhibits hair shaft elongation (Peters et al, 2007).
Diagnosis and differential
A thorough history and physical exam is typically enough to make a diagnosis of TE (Hughes & Saleh, 2021). The most common scenario is presented is an abrupt onset of hair shedding with little to no other symptoms. One must be diligent to question potential causative events 3-6 months prior to the onset of hair shedding(Hughes & Saleh, 2021). The clinician can opt to perform a pull test, which may or may not yield positive results. A positive test is at least 4 hairs removed with each pull (Hughes & Saleh, 2021).
If there is concern of other co-morbidities (e.g. hyperthyroidism or iron deficiency) either causing or aggravating the hair loss, further testing may be indicated (Hughes & Saleh, 2021). The differential diagnoses list can include: Alopecia Areata; Anagen Effluvium; Androgenetic Alopecia, Scarring Alopecia, Syphilis; and Trichotillomania (Hughes & Saleh, 2021).
Prognosis and treatment
TE is a self-limiting condition that typically lasts about 6 months (Peters et al, 2006). When deciding how to proceed with treatment strategies, it is key to review the patient’s history and to determine whether the initial stressor was metabolic, hormonal, lifestyle/environmental, or due to medication. If the initial stressor has either been removed or treated, there is little need to use additional therapies (Hughes & Saleh, 2021). Conventional hair growth treatments are typically not used in cases of TE, however, the patient can choose to apply topical minoxidil (Hughes & Saleh, 2015).
When treating a TE patient using the Naturopathic approach, the emphasis shifts towards supporting the adrenal glands and regulating the HPA axis. Additionally, it is imperative to review key foundational aspects of the patient’s lifestyle such as stress management/restoration techniques, reducing inflammation, improving diet and correcting nutritional imbalances, and improving the quality of sleep.
A class of herbs that is particularly useful in the treatment of TE are adaptogenic herbs. One of the best studied adaptogenic herbs is Ashwagandha, or Withania somnifera (Chandrasekhar et al, 2012). In a randomized, double-blind, placebo-controlled study, it was found that supplementing with 300 mg of Ashwagandha twice daily for 60 days significantly reduced scores on the Perceived Stress Scale, improved scores on the General Health Questionnaire-29, and Depression Anxiety Stress Scale, and reduced cortisol levels (Chandrasekhar et al, 2012). Another adaptogenic herb that may play a role in hair growth is ginseng (Choi et al, 2018). Ginseng has the potential to promote hair growth and prevent hair loss by encouraging the anagen stage while inhibiting the catagen stage (Truong et al, 2017).
An emerging treatment for hair loss, TE and otherwise, is low level laser therapy (LLLT) (Avci, et al, 2014). Low-level laser therapy stimulates cellular activity, while near-infrared laser light promotes regeneration (Avci et al, 2014). Commonly used devices have wavelengths in the 500-1100 nm range, with most evidence pointing towards 655 nm as target wavelength (Amer et al, 2021). LLLT has been found to be safe and effective in both animal studies (Avci, et al, 2014) and human studies, in both males and females (Yoon et al, 2020).
Summary
Telogen effluvium is a short-term, self-limiting condition in which there is diffuse hair loss after a stressful event. The interplay between various stress hormones has been directly implicated in the condition, as they both inhibit the growth of hair and speed up the transition from growth to rest phase. Since TE is self-limiting, treatment is not necessary. If the patient, however, desires a more hands-on approach, there are various conventional and naturopathic treatment options that can target hair growth and support and restore the body’s ability to handle stress.
Dr. Esha Singh is a naturopathic doctor practicing in Vancouver, BC. She has a clinical focus in skin health and uses an integrative approach to clinical dermatology. Dr. Esha strives to make information skin health and wellness simple and accessible.
Print this page